
Morphological Music Therapy is an approach that has been developed in Germany for 25 years. It is based on old European scientific traditions, especially on the scientific approach of Goethe. In its modern form, it includes insights from psychoanalysis and Gestalt psychology and has developed methods for qualitative research in music therapy (Tüpker 2002, Weymann 2000a). In Germany this approach is taught at several university music therapy trainings and a number of books and articles have been published.
Müsset im Naturbetrachten
immer eins wie alles achten.
Nichts ist drinnen, nichts ist draussen,
denn was innen, das ist außen.
So ergreifet ohne Säumnis
Heilig öffentlich’ Geheimnis.
Erfreuet Euch des wahren Scheins,
Euch des ernsten Spieles
denn nichts Lebendiges ist eins,
immer ist’s ein Vieles.
You must, when contemplating nature,
Attend to this, in each and every feature:
There’s nought outside and nought within,
For she is inside out and outside in.
Thus will you grasp, with no delay,
The holy secret, clear as day.
Take joy in true appearance,
And in serious play,
For no living being is singular,
But always a plurality.
Goethe—“Epirrhema” (1821)
Morphology (from Greek morphe, meaning form, shape) refers to the study or knowledge of forms or shapes. The objects of morphological research are investigated from the perspective of their formation, their structure, and their changes of form (metamorphosis). Today the term morphology is used in disciplines as diverse as psychology, geology, biology, and linguistics. Occasionally the term is used in a limited way to refer only to set structures or the results of a process of formation. At other times, as in this chapter, the formation process itself is examined and may even be the focus of interest.
In music therapy the entire therapeutic process (music, conversations, emotions, behavior, etc.) can be thought of as a gestalt formation and be related to other relevant gestalt formations in the patient (biography, organization of daily life, symptoms, etc.). This is primarily a psychological perspective, since it is related to formations of the psyche, but it includes musicological perspectives also. To think about music as a psychological object means above all to investigate it from an experiential aspect, that is, to understand it as a gestalt of effects.
Under the premise that psychological data can only be obtained through the reflected subjectivity of the researcher, experiential description became the most important instrument of knowledge in morphology, integrated into varied methodological contexts such as the in-depth interview and the experiential record. “The description of complete contexts becomes the basic method of psychological morphology because no isolated facts or data as such exist outside of the object-oriented living context” (Salber, 1991, p. 52). “Description seeks to grasp the movement of phenomenal forms”[1] (Salber, 1969, p. 63), which then have to be transformed into explanatory reconstructions through several intermediate steps. Aside from developing and reflecting upon therapeutic concepts, the main foci of morphological psychological research are psychological factors of everyday life, psychology of the arts and the new media, and commercial and business psychology. Research results are published in the journal Zwischenschritte (Intermediate Steps) and elsewhere.
Some music therapists became interested in morphological psychology in the 1970s because of its affinity with art and the psychology of the arts. In 1980, Frank Grootaers, Tilman Weber, and the authors of this chapter established a research group for the morphology of music therapy and then later, in 1988, the Institute for Music Therapy and Morphology (IMM). In this institute, the basic ideas of morphological music therapy were developed as an integration of research and practice. The initial goal was to use concepts from morphological psychology to make description of the music therapy process possible, and to develop music therapy-specific procedures to enable their scientific reconstruction. In this context, the investigation of improvisation in music therapy is of special significance. The results were disseminated through numerous professional conferences, courses, and publications, as well as in a series called Materialien zur Musiktherapie (Studies of Music Therapy). Morphological music therapy is taught at the University of Münster and the Hamburg University of Music and Drama.
The term morphology goes back as far as the German poet and scientist J. W. Goethe (1749–1832), who proclaimed a scientific view expressly set against the (then current) mainstream of positivist and reductionist positions. He turned against the prevailing opinion that the knowledge of nature was to be found only by dissection and analysis, by an identification of ever-smaller pieces. Instead, he sought to understand characteristic features of “organic natures” in a holistic manner, using principles such as formation and transformation, including both spatial and temporal dimensions. In this way he tried to gain “insight into the context of their essence and actions”[2] (Goethe, 1954, p. 6). He described these contexts, derived by thorough observation of individual cases, as types or formation principles (ur or primeval phenomena). With these ideas, Goethe placed himself in the tradition of Aristotle’s empirical (based on experience) philosophy of nature, according to which living forms are subject to growth and loss. This philosophy views living forms as historical phenomena, emphasizing aspects of development and process. Thus, Goethe (as well as Aristotle) could be called a forerunner of modern qualitative research strategies (see Harlan, 2002; Mayring, 1986).
Goethe developed his concept of morphology beginning in 1790 in different scientific subjects (anatomy, botany, theory of colors, etc.). He characterized it distinctly in his programmatic introduction About Morphology, written in 1817, as the science of “formation and transformation of organic natures” (Goethe, 1954, p. 2).[3] These living organic natures were always regarded both as having/being form and being changeable.
The morphologist attempts to graphically convey the experience of and create a systematic reconstruction of whatever phenomenon or living object is the focus of interest and perception. According to Goethe, theory develops from unmediated vivid experience and is not found behind or beyond the level of phenomena. In the process of perception, we already actively begin to theorize and systematize—or, more to the point, we form, shape, or reorganize. The gestalt concept connects phenomenon, perception, and theoretical reconstruction: All are understood both to be and to have form. In Goethe’s (1965) terms: “Gestalt is something that moves, becoming and diminishing. Knowledge of gestalt is the knowledge of metamorphosis” (p. 128). In this definition of the gestalt concept, the developmental approach of morphology becomes clear.
Morphological psychology, established by Wilhelm Salber in the 1950s, takes up this gestalt concept against a background of considerations from gestalt psychology and psychoanalysis. In morphological psychology, the psyche and its essence are conceptualized as a gestalt formation and at the same time as a transitory event between gestalt and transformation. Experience and behavior are functions of this overall process. Within the flow of the reality of formations of the psyche, morphological psychology strives for principles of organization, for blueprints and inherent laws. It attempts to work out the moving system of the life of the psyche. The life of the psyche resembles a traveling figure[4] (Salber, 1991), a guiding metaphor of morphological psychology. This view attributes to the life of the psyche a special affinity towards the arts. “The marriage of science and art sets a cognitive process in motion where art und science can learn from each other” (Tüpker, 2001, p. 57).
The decision to use a specific methodology is based on preconceived notions about the type, composition, and limitations of the object of research. An object with a certain prescientific or everyday meaning becomes a scientific object.[5] Using the instruments and procedures of morphological psychology, diverse phenomena are viewed and conceptualized as psychological phenomena, as productions of the psyche. Therefore, the main objective of morphological research is the exploration of psychological processes as they emerge from experience and behavior. One approach involves structural analysis of verbalizations of different (self-) observations. These are then reconstructed in several interrelated hermeneutic steps. The objective in each case is to reconstruct the interplay of those gestalt factors or structures of experience involved in the experiential situation under investigation. The psychological event is reconstructed as a dramatic interplay, as an interlocking of several polarities within the process.
The morphological research process unfolds its object suspended between phenomenon and interpretation. A constant shifting of perspectives is characteristic. Every data collection is the result of choosing (and excluding), sorting, or forming. It is motivated by a specific search, a vague pre-knowledge or preconception of the whole. Neither pure facts nor complete objectivity exist. Morphological research always involves reconstruction.
A typical morphological course of research can be demonstrated from four different versions or perspectives that organize the process. The method of the steps is based on the general idea that a psychological wholeness[6] can only be represented (reconstructed) in a sufficiently complete and complex way if it is described repeatedly and from different perspectives. These four perspectives can be equally applied to the therapy process and case descriptions as to the research process in a modified form (for more detail see Tüpker, 2001, pp. 60–70; Tüpker, 2004).
Morphology offers several systems that make this theoretical orientation possible. For research in music therapy, the system of the six gestalt factors (Tüpker, 1988/1996a) and the concept of primary and secondary figuration (e.g., Grootaers, 2001; Weymann, 2004) have been used.
As an illustration of two possible perspectives that morphological research can bring to understanding treatment and research processes, one example of treatment steps and one of research steps are presented below. These are only two of many possible examples of how these perspectives can be applied.
As steps or aspects of treatment, the system of the four versions or perspectives can be used on two levels: (a) to help to structure the treatment or to develop a special treatment concept, or (b) to analyze and evaluate a course of treatment after it is completed (as might be done for research purposes). Going through all four steps is the qualitative criterion, with its specific application being based on the individual project that is being researched as well as its general set-up. The treatment steps can be used either to describe the entire development of a treatment or to analyze an individual session.
Step 1. Leiden-Können[7] or Treatment Objectives. The first treatment step represents treatment objectives and thus corresponds to diagnosis in music therapy. However, whereas in medicine diagnosis and indication formally precede treatment, in psychotherapy they are part of treatment and may develop and change in the course of treatment. The technical term from morphological psychology, Leiden-Können, refers to several things simultaneously. It refers to what the patient complains about as the source of emotional and physical suffering, but also under what circumstances she or he suffers. In the same way, we are interested in the patient’s skills, abilities, and resources and in what she or he likes and dislikes.[8] We also go on the assumption that the patient might possibly like what she or he complains about even more than that from which she or he must protect him- or herself through the emotional constructions. All this is explored in both the patient’s narrations and the music. In order to do this, the description and reconstruction that are described below may be applied as a diagnostic instrument. Leiden-Können changes within the course of treatment, not just as progress is made in treatment but also as deeper layers of suffering become apparent.
Step 2. Methodifying. The second treatment step refers on the one hand to the therapist following methodical principles of treatment. On the other hand, we assume that patients will follow a method as well in the sense that they treat the treatment situation, the therapeutic relationship, and the music in the same way that they deal with themselves and the world. In this way patients transfer their method of living to the treatment situation and also involve the therapist in this event. This is all the more so when the therapist gets involved in the interplay of transference and countertransference. Like modern psychoanalysis, morphological music therapy assumes that it is part of the therapist’s methodological task to become empathically involved by being moved. Then, by again acquiring some distance, the therapist’s empathy leads to understanding. This understanding may then be communicated to the patient, either symbolically (in music or play) or by means of verbal interpretation. Thus becoming methodological connects the participants and speeds up the development of treatment.
Step 3. Changing. With the concept of changing (transformation), we look for changed experiences in treatment, a new viewpoint, a different tone in the music, a new way of expression. Through these, transformation and restructuring within the patient’s method of living may announce themselves. Such turning points can become evident when connected with an aha experience, a sudden insight, a jolt in the psyche. Changes can also take place almost unnoticed and become more evident in retrospect. Changing is the internal criterion for the effects of the treatment, such as the effects of therapist’s interpretations or of musical interventions. If those elements are missing, we must ask ourselves what must be changed methodologically and why the methodological procedures have not worked so far.
Step 4. Implementation.[9] In the last step we look at the changes that reach beyond the treatment setting: What does the patient put into action in her or his everyday life? What is he or she able to implement? How is he or she able to deal with daily life differently? Part of this is, of course: How do her or his symptoms, complaints, and suffering improve, or how does the treatment improve her or his quality of life?
A scientific procedure called Description and Reconstruction, originally developed for analyzing improvisations in music therapy (Tüpker, 1996a), is frequently used. It enables us to focus on the musical part of music therapy as the center and starting point for scientific (as well as musical) considerations. Diagnosis and the evaluation of therapy can consequently be done in a music-centered way (Weymann, 2000b).
It is our aim to work out the gestalts of effects in improvisations. Assuming that their musical structures correspond to those of the psyche, we wish to explore those characteristic patterns in improvisations, which, as psychic structures (method of living), are also connected to the patient’s disorder or dilemma.
Through these four methodological steps, the above-mentioned versions can be clearly identified. This procedure may be applied to different subjects and contexts of research and is based on the effect of the musical experience. In this regard, it is similar to other comparable methodological approaches from the sphere of in-depth hermeneutic procedures (see also Langenberg et al., 1996; Metzner, 2000)
As part of the first step, experiential descriptions of the music are made. This is done by a group of trained experts who listen to the audio recording without having any other case information. The subsequent steps are then developed by the researcher, who usually also is the therapist of the case study, along the guidelines of the summarized text.
The four methodological steps (which on the whole perform a hermeneutic spiral), summarized in Table 1, will subsequently be illustrated through excerpts from a case study. (For a detailed example that uses all the steps in a case study see Irle, 1996.)
Table 1
Methodological Steps: Description and Reconstruction
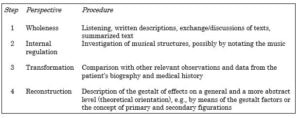
Step 1. Wholeness. The describers focus their attention on the phenomenon with an unprejudiced attitude and a willingness to be moved by it. They are asked to write notes in a simple and comprehensible language. The descriptions are read aloud and compared with an eye to common factors or differences. The discussion within the describer’s group aims at the formulation of a summarized text, which should also include possible contradictions and countertendencies and thus often represents something like a formulation of the problem. The following excerpt from the description of one person provides an example:
Something must be done very fast. No pauses. Stillness is dangerous, on and on. I cannot stop. There is a stumbling somewhere inside there. I’ve got to get away. I’m running, but something always holds me back; shouldn’t I rather stay? No, I have no time to linger. . . almost unbearable longing.
Common to all descriptions was the symptom of restlessness, a restless movement that has no ending and therefore seems without purpose. In a counter-movement, the existence of obstacles is emphasized: stumbling, something holds me back, etc. Everything seems to be kept in suspension, although this becomes almost unbearable. After some discussion the group finally agreed on the following summarized sentence:
Something that’s being driven is continuously held up and never arrives. The result is a tormenting suspense.
Step 2. Internal Regulation. Working from the summarized text, we develop questions and follow up with a selective detailed analysis of the music. We investigate relevant examples on the basis of the recording and possibly the notation, as to how the described impression is created in sound. Through this, particular features of the musical structure are worked out. These may then be used as evidence and specification of the experiential gestalt and moreover as an indication of the (subconscious) method of its production. Here, the relationship of part-to-whole is investigated, in the sense of a hermeneutic approach. For example:
How is the impression of suspense achieved, of being driven and at the same time being stopped? What constellation of musical parameters creates the image of not-arriving?
This can be demonstrated in the example through the rhythmic features. From the very beginning, the impression of the unexpected, the unpredictable, is created. The rhythms seem to be put together from many snippets. The first three notes seem to establish the pulse, but the fourth comes too early by comparison. This could be a syncopation, if the connection to the pulse were reestablished at some point. Instead, more breaks follow, but always just missing what is expected, creating an impression of suspense.
Step 3. Transformation. In the third step the research unit is broadened, again along the guideline of the theme gained so far, by including data from other sources: notes from the therapy process, from the case history, the patient’s biography, his everyday narrations and dreams. Thereby the picture is enriched but is also corrected. But most of all we discover indications about the importance and the secret meaning of the observed gestalt formation within the patient’s life context. Through the variation the structural element is also emphasized. For example:
The patient, a 24-year-old man, suffers from a severe compulsion with obsessive washing and control compulsions. He feels constantly tormented by doubts, rendering him almost completely incapable of making decisions in his daily life. For instance, he cannot just sit down in a chair but hesitates for a while between a standing and a sitting position, as if in suspense. He tries to avoid leaving any traces or feeling impressed by anything.
Step 4. Reconstruction. The reconstruction seeks to lead the gestalt that was found back to basic conditions of emotional life, for instance the interplay of factors of the psyche. Thus, on a structural level, the internal logic of the phenomenon can be represented as a kind of moving pattern from which indications about the patient’s subconscious life organization, or about his individual gestalt formation, can be deduced. For example:
The gestalt factors of arrangement and effect do not form a complementary relationship with each other but create a short circuit, as it were. The beginnings of formation are incessantly subjected to sorting procedures; these seem unachievable by any other limiting tendency. Thus, actions are initiated but then inhibited and cannot be completed. At the same time, the sorting tendency does not unfold because no distinctive gestalt is formed, leading to disorganization.
The methods resulting from the above-mentioned fundamental ideas of morphology show numerous factors common to other types of qualitative research. These factors include reflexivity, an idiographic approach, and the interpretive paradigm that takes its starting point from the researcher’s reflected subjectivity.
Methodologically, the affinity to the hermeneutic approach is particularly noticeable. The postulate of an experiential moving along together[10] with the living research object determines a procedural and somewhat phenomenal approach to reality. Through several intermediate steps, this approach approximates the level of theory and thus also the possibility of understanding and explaining the phenomena. Since unconscious determinants are also included, one could also call it an in-depth hermeneutic approach in the sense of Lorenzer (1986). A synthesizing basic feature is characteristic of a morphological research process: the search for a context substantiated by analytical working steps. In this we recognize similarities with the heuristic procedures of art, a connection that in morphology is termed psycho-aesthetics or an art-analogous procedure.
Apart from psychoanalysis and gestalt theory, we also recognize a special affinity with systemic thought (Watzlawick, 1976) on the level of models and theories (gestalt factors, versions, part-whole relationship, gestalts, and transformation).
Morphological music therapy research includes practical and methodological questions, as well as broader questions that are concerned with music, therapy, health, illness, and society. More specialized areas are classified into: (a) individual case and group studies, (b) comparative studies, and (c) music psychology. A selective overview of studies and results to date on the basis of this classification follows.
The morphological scientific procedure Description and Reconstruction, described above, is applied most frequently. There are about 100 examples of this diagnostically oriented research procedure (in some cases as yet unpublished). Almost the whole scope of music therapy is found wherever free improvisation, in the broadest sense, is used. For other areas, some partly modified procedures have been developed (Spliethoff, 1994), and a specially modified form for group analysis may be found in Grootaers (2001). Apart from analysis on the basis of gestalt factors, other reference systems, such as psychoanalytic pathology or developmental psychology (Irle & Müller, 1996), may be chosen for the theoretical orientation. On a pragmatic level, it is possible to apply morphological procedures without fully understanding principles of morphology. This is of special interest because we have found that description itself (included in step 1 of the Description and Reconstruction procedures), even in nonscientific contexts such as supervision or practice-related quality assurance, allows a more in-depth and elucidating view of the individual case, which improves the treatment. The music therapist is thus in the position to make an important contribution to the treatment team toward understanding the patient by translating the results of musical communication with the patient into psychological language.
Naturally the results of such individual case studies can only be summarized in a very general way. The results of these studies allow us to state: Irrespective of the patient’s musical background and under certain preconditions with regard to the therapeutic setting, fundamental structures of the psyche can be expressed by improvising with the therapist. These are also related to the patient’s disorder or conflict situation. They can be described and objectified by independent observers through their manifestation as musical structures, thus contributing to the comprehensive psychological understanding of the patient by complementing the language-limited approach to patient care.
The method of analyzing the course of treatment presented here (treatment steps) has been used in about 30 case studies or short presentations to verify the sequence of events in treatment. The results differ from case to case because of different treatment conditions that make comparison difficult. Not only do the very diverse reasons for therapy play a role, but external conditions beyond the control of the music therapist also make a difference. These include such factors as financial restrictions on treatment, legal restrictions on outpatient music therapy, and a lack of options for patients. We can state, though, that in those music therapy treatments that were not too heavily restricted by exterior conditions, a complete cycle of the four steps of treatment was achieved, which methodologically could be considered a successful treatment. Individually, the respective preconditions are too diverse for us to formulate an overall result. One exception is the study by Grootaers (2001) in which 13 individual and 2 group studies in psychosomatic care, based on the four treatment steps, show in detail the success of a music therapy treatment in favorable and comparable inpatient conditions. There the relevant turning figure is worked out for every patient individually, so that the success of the treatment is oriented toward and measured by the individual patient’s method of living, disorder, and living situation.
Comparative studies include papers in which morphological methods themselves are reviewed and further developed by means of comparative observation.
In one study (Mömesheim, 1999), the 171 texts created through Description and Reconstruction procedures were investigated using methods from literary studies. The researcher developed criteria for text analysis that were then used for further comparative research. She found that in all 26 descriptions there was a verifiable connection between the established gestalt of effects of the improvisation (research step 1) and the musical formation of forms (step 2). In addition, the researcher made detailed recommendations as to the formulation of the gestalt of effects as well as the development of the gestalt formation. These recommendations were made on the basis of qualitative differences within the comprehensibility of individual contexts, the summary generalization, and internal regulation.
Hülsmann (2002) compared two morphological descriptive procedures, one with an external group of describers (Tüpker, 1988/1996a) and the other with a description by patients (Grootaers, 2001), on the basis of examples of music in group music therapy. Certain clearly discernable common factors emerged, and these are regarded as proof of the validity of both procedures. The obvious differences may be psychologically explained on the grounds of individual perspectives (self-involvement/distance, awareness/lack of awareness of temporal developments, and other events in the group) and constitute a supplementary relationship.
Another group of studies includes studies in which patients’ initial improvisations are compared to comparable diagnoses in terms of their psychological gestalts of effects and their musical gestalt formation. To this date, comparative studies of patients with chronic pain (Krapf, 2001; Tüpker, 2002, pp. 56–67), borderline personality disorder (Tönnies, 2002), and anorexia (Erhardt, 2003; Kang-Ritter, 2003) are available. To varying degrees, common factors were demonstrated in the way these groups of patients expressed themselves. For instance, many more common factors emerged with patients with pain than with those with borderline personality disorder or anorexia. However, new insights were gained about the understanding of these disorders as well as some clues for music therapy treatment.
On the basis of the four treatment steps, Haubitz (1999) compared the development of two group treatments with depressive patients. In the music, as well as in transference and countertransference, the differences between one group of patients with more neuroses and another group with psychoses were clearly observed.
Other issues are worked out in comparative studies that relate to general aspects of treatment. Methodologically, these studies overlap to some degree with the aforementioned area. Based on interviews, Mönter (1998) compared the proportions of verbal conversations in music therapy and systematized the results using the four versions (based on 12 explorative expert interviews). Music therapy publications are the subject of two other comparative studies investigating the beginning (Krückeberg, 2000) and the ending (Stihl, 2000) of music therapy treatment. Wältring-Mertens (1999) compared 40 case histories based on the question of the practical significance of music in music therapy with children. This study shows a multitude of music-related event forms, emphasizing flexibility and openness as characteristic features of music therapy with children.
By means of the methodological evaluation of qualitative interviews (in-depth interviews, explorative expert interviews) and other qualitative interview methods (such as semi-structured questionnaires), general questions related to music therapy such as the experience of music therapy supervision (Schmutte, 2002; Tüpker, 1996b) can be explored, as well as basic issues about the psychology of musical experience and activity outside of the therapy context. Studies to date are concerned with questions of improvisation (Domnich, 1995; Leikert, 1990; Weymann, 2004), singing (Wachwitz-Homering, 1993), the relationship between player and instrument (Meyer, 1992), or practicing an instrument (West, 1992). There are no clear-cut differences between those papers with a morphological orientation and other related psychological approaches.
As one example, we will examine more closely the dissertation of Weymann (2004). It deals with the question of “how life’s work and the activity of improvisation are related to one another. How does the method of living manifest in dealing with improvisation? How does this indicate specific characteristics and implications of the improvisation activity?” (p. 53). For this purpose, 12 in-depth interviews were conducted with musicians in whose lives improvisation plays an emotionally significant role. The basic conditions were first worked out individually. These may be described as different forms of a polarity around the central theme of transformation versus identity (p. 192). As soon as the transformation became evident as the primary figuration (in the form of: stimulating, dissolving, delimiting, shifting, going beyond, letting go, being swept along in an intoxicated way, united/going beyond one’s own space, rough/unfinished), the opposite pole appeared in the secondary figuration (as anchoring, unifying, securing, framing, integrating, controlling, being opposite, different, developed/elaborated; pp. 189–191). By contrast, in a second group, aspects of finding one’s identity through improvisation were initially emphasized with these words: assertion, alone, finding oneself. Here too, the opposite pole appeared in the secondary figuration (canceling, united, sharing).
The final typical solutions that were worked out with regard to the established polarity in the sense of a self-treatment through music “represent. . . examples in the sense of pre-images or prototypes which may serve as guideposts for the concrete gestalt formation in real-life practice of music therapy” (Weymann, 2004, p. 207).
[1] The sources for this and other quotations are in German but have been translated to English as cited here. The original German is given only when it provides information that is not apparent in the translation.
[2] Original: Einsicht in den Zusammenhang ihres Wesens und Wirkens
[3] Bildung und Umbildung organischer Naturen
[4] Gestalt auf Reisen
[5] Gegenstandsbildung (formation of the scientific object)
[6] Ganzheit
[7] To suffer, to be able to
[8] The German word leiden not only means to suffer but also to like something. Etymologically it is linked to the meaning of traveling and gaining experience.
[9] The German word Bewerkstelligen, containing the word Werk, emphasizes the product character of this last step as well as the process.
[10] Mitbewegung
Domnich, C. (1995). Untersuchung zur freien musikalischen Improvisation als Gestaltungsversuch des Seelischen [An exploration of free music improvisation as emotional gestalt]. Unpublished music therapy diploma thesis, Münster University, Münster, Germany.
Erhardt, C. (2003). Hunger nach Weniger. Vergleichende Untersuchung musiktherapeutischer Erstimprovisationen magersüchtiger Patienten [The hunger for less: A comparison of initial improvisations of anorexic patients in music therapy]. Unpublished music therapy diploma thesis, Münster University, Münster.
Goethe, J. W. von (1954). Bildung und Umbildung organischer Naturen. Die Schriften zur Naturwissenschaft (Leopoldina-Ausgabe). Erste Abteilung, Band 9 [Formation and transformation of organic natures. Writings on natural science (Leopoldina Edition). 1st section, Vol. 9]. Weimar, Germany: Böhlau.
Goethe, J. W. von (1965). Die Schriften zur Naturwissenschaft (Leopoldina-Ausgabe). Erste Abteilung, Band 10 [Writings on natural sciences (Leopoldina Edition). 1st section, Vol. 10]. Weimar: Böhlau.
Grootaers, F. G. (2001). Bilder behandeln Bilder: Musiktherapie als angewandte Morphologie [Images treat images: Music therapy as applied morphology]. Münster: Lit-Verlag.
Harlan, V. (2002). Das Bild der Pflanze in Wissenschaft und Kunst [The image of plants in science and art]. Stuttgart, Germany: Mayer.
Haubitz, S. (1999). Vergleichende Untersuchung zweier Musiktherapiegruppen in der Psychiatrie [Comparative study of two music therapy groups in psychiatry]. Unpublished music therapy diploma thesis, Münster University, Münster.
Hülsmann, M. (2002). Vergleichende Untersuchung von zwei morphologischen Beschreibungsverfahren [Comparative study of two morphological descriptive processes]. Unpublished music therapy diploma thesis, Münster University, Münster.
Irle, B. (1996). Der Spielraum Musiktherapie als Ergänzung des padagogischen Auftrages in einem Internat [The music therapy playroom as an educational augmentation in boarding school]. In B. Irle & I. Müller (Eds.), Raum zum Spielen—Raum zum Verstehen. Musiktherapie mit Kindern (pp. 10–102). Münster: Lit-Verlag.
Irle, B., & Müller, I. (1996). Raum zum Spielen—Raum zum Verstehen. Musiktherapie mit Kindern [Room to play—room to understand. Music therapy with children]. Münster: Lit-Verlag.
Kang-Ritter, A. (2003). Musiktherapie mit essgestörten Kindern und Jugendlichen. Eine vergleichende Untersuchung von Beschreibungstexten musiktherapeutischer Improvisationen [Music therapy for children with eating disorders: A comparative study of descriptions of initial improvisations in music therapy]. Unpublished music therapy diploma thesis, Münster University, Münster.
Krapf, J. M. (2001). Auf den Schmerz hören. Vergleichende Untersuchung der musikalischen Erstimprovisationen von chronischen Schmerzpatienten [Listening to the pain: A comparative study of initial music improvisations by patients with chronic pain]. Unpublished music therapy diploma thesis, Münster University, Münster.
Krückeberg, W. (2000). Zum Beginn musiktherapeutischer Behandlungen [Beginning music therapy treatment]. Unpublished music therapy diploma thesis, Münster University, Münster.
Langenberg, M., Frommer, J., & Langenbach, M. (1996). Fusion and separation: Experiencing opposites in music, music therapy, and music therapy research. In M. Langenberg, K. Aigen, & J. Frommer (Eds.). Qualitative music therapy research: Beginning dialogues (pp. 131–160). Gilsum, NH: Barcelona Publishers.
Leikert, S. (1990) Die Lust am Zuviel—Der Wirkungsraum der Instrumentalimprovisation [The pleasure in overabundance—The “effect area” of instrumental improvisation]. Zwischenschritte, 2, 27–39.
Lorenzer, A. (1986). Tiefenhermeneutische Kulturanalyse [In-depth hermeneutic cultural analysis]. In A. Lorenzer (Ed.), Kultur-Analysen (pp. 11–98). Frankfurt, Germany: Suhrkamp.
Mayring, P. (1986). Einführung in die qualitative Sozialforschung [An introduction to qualitative social research] (2nd ed.). Weinheim, Germany: Beltz.
Meyer, B. (1992). Instrument und MusikerIn—Psychologische Aspekte einer Beziehung [Instrument and musician: Psychological aspects of a relationship]. Unpublished music therapy diploma thesis, Münster University, Münster.
Metzner, S. (2000). Ein Traum: Eine fremde Sprache kennen, ohne sie zu verstehen. Zur Evaluation von Gruppenimprovisationen [A dream: to know a foreign language, without understanding it. Evaluating group improvisations]. Musiktherapeutische Umschau, 21, 234–247.
Mömesheim, E. (1999). “Wer verschweigt das letzte Wort?”—Vergleichende Untersuchung von Beschreibungstexten aus der Morphologischen Musiktherapie [Who conceals the last word? A comparative study of descriptive texts in morphological music therapy]. Unpublished music therapy diploma thesis, Münster University, Münster.
Mönter, U. (1998). Das Gespräch in der Musiktherapie [Discussion in music therapy]. Musiktherapeutische Umschau, 21, 5–22.
Salber, W. (1969). Wirkungseinheiten [Effect units]. Cologne, Germany: Moll und Hülser.
Salber, W. (1991). Gestalt auf Reisen [Traveling figure]. Bonn: Bouvier.
Schmutte, M. (2002). Supervision in der Musiktherapie—Erlebensweisen, Erfahrungen und Einschätzungen von Supervisanden [Supervision in music therapy: Experiences and estimations of supervisors]. Unpublished music therapy diploma thesis, Münster University, Münster.
Spliethoff, G. (1994). Untersuchung seelischer Gestaltbildungen auf dem Hintergrund musiktherapeutischer Erfahrungen mit geistig Behinderten [An exploration of emotional gestalt formations on the background of music therapy experiences with the mentally handicapped]. Unpublished music therapy diploma thesis, Münster University, Münster.
Stihl, C. (2000). Die letzte Musiktherapiestunde—Abschied und neuer Anfang [The last music therapy session: closure and new beginning]. Unpublished music therapy diploma thesis, Münster University, Münster.
Tönnies, F. (2002). Erstimprovisationen von Borderline-Patienten. Eine vergleichende musikalisch-psychologische Untersuchung [Initial improvisations of borderline patients. A comparative music-psychological exploration]. Unpublished music therapy diploma thesis, Münster University, Münster.
Tüpker, R. (1996a). Ich singe, was ich nicht sagen kann. Zu einer morphologischen Grundlegung der Musiktherapie [I sing what I cannot say. A morphological foundation of music therapy] (2nd ed.). Münster: Lit-Verlag. (1st edition published 1988).
Tüpker, R. (1996b). Supervision als Unterrichtsfach in der musiktherapeutischen Ausbildung [Supervision as a course in music therapy education]. Musiktherapeutische Umschau, 17, 242–251.
Tüpker, R. (2001). Morphologisch orientierte Musiktherapie [Morphologically oriented music therapy]. In H-H. Decker-Voigt (Ed.). Schulen der Musiktherapie, 55–77. Munich, Germany: E. Reinhardt.
Tüpker, R. (2002). Forschen oder Heilen. Kritische Betrachtungen zum herrschenden Forschungsparadigma [To research or to heal. Critical observations of the dominant research paradigm]. In P. Petersen (Ed.), Forschungsmethoden künstlerischer Therapien (pp. 33–68). Stuttgart: Mayer
Tüpker, R. (2004). Morphological Music Therapy. Nordic Journal of Music Therapy, 13, 82–92.
Wachwitz-Homering, (1993). Untersuchung zur Wirkungseinheit des Singens [An exploration of the “effect unit” of singing]. Unpublished music therapy diploma thesis, Münster University, Münster.
Wältring-Mertens, B. (1999). Zur Bedeutung der Musik in der Musiktherapie mit Kindern [The meaning of music in music therapy with children]. Unpublished music therapy diploma thesis, Münster University, Münster.
Watzlawick, P. (1976). Wie wirklich ist die Wirklichkeit? Wahn—Täuschung—Verstehen [How real is reality? Illusion—deception—understanding]. Munich: Piper.
Weymann, E. (2000a). Sensitive suspense: Experiences in musical improvisation. Nordic Journal of Music Therapy, 9, 38–45.
Weymann, E. (2000b). Indications of the new: Improvisation as a means of inquiry and as an object of research. Nordic Journal of Music Therapy, 9, 55–66.
Weymann, E. (2004). Zwischentöne. Psychologische Untersuchungen zur musikalischen Improvisation [Intermediate tones. Psychological explorations of music improvisations]. Gießen, Germany: Psychosozial Verlag.
West, U. (1992). Psychologische Untersuchung über Einübungsprozesse beim Musizieren [A psychological exploration of practice processes in making music]. Unpublished diploma thesis, Cologne University, Cologne.

Musiktherapeutin, Morphologin, Märchenforscherin
Prof. Dr. phil. Rosemarie Tüpker, Jahrgang 1952, studierte zunächst Musik an der Musikhochschule Köln und anschließend Musikwissenschaft, Psychologie und Philosophie an der Universität zu Köln. Dort lernte sie Wilhelm Salber und seine Morphologie kennen. Fasziniert von der Kunstnähe dieser Psychologie brachte sie die Morphologie in die Musiktherapieausbildung ein, die sie parallel im Mentorenkurs Musiktherapie in Herdecke absolvierte. Mit musiktherapeutischen Kollegen gründete sie die Forschungsgruppe und das Institut zur Morphologie der Musiktherapie, welches die Morphologie in Musik und Therapie erforschte und lehrte. Nach einer Zeit als Musiktherapeutin in einer psychosomatischen Klinik leitete sie von1990 bis 2017 die Studiengänge Musiktherapie an der Universität Münster. Ihre Forschungsschwerpunkte liegen im Schnittfeld von Morphologie, Psychoanalyse, Künstlerischen Therapien, Wissenschaftstheorie und Märchenforschung.
Website: https://www.rosemarietuepker.de
